
•Overview
Understanding the Condition
Ehlers-Danlos Syndrome (EDS) is a group of heritable connective tissue disorders caused by genetic variants that affect the structure, production, or processing of collagen and related proteins. Because connective tissue serves as the body's structural framework — supporting skin, joints, blood vessels, and internal organs — EDS can produce symptoms across virtually every body system, making it one of the most complex and multisystemic conditions in medicine.
The 2017 International Classification recognizes 13 distinct subtypes of EDS, each with its own genetic basis and clinical profile. The most common is hypermobile EDS (hEDS), which affects the majority of patients. Vascular EDS (vEDS) is the most serious subtype, carrying risk of life-threatening arterial or organ rupture.
Hypermobility Spectrum Disorder (HSD) is a closely related condition diagnosed when joint hypermobility causes pain, instability, and functional impairment, but the full diagnostic criteria for EDS are not met. HSD and hEDS share significant clinical overlap and are now understood to exist on a continuum.
EDS and HSD are far more prevalent than previously recognized and are frequently underdiagnosed or misdiagnosed — sometimes for decades. Patients are often told their symptoms are due to anxiety, fibromyalgia, or simply "being flexible" before finally receiving an accurate diagnosis.
•Recognition
Signs and Symptoms
Many symptoms overlap across EDS subtypes and HSD due to their shared connective tissue involvement. Severity and combination of symptoms vary considerably by subtype and individual.
Skin
Hyperelastic (stretchy) skin, fragile skin prone to tearing and bruising, slow wound healing, atrophic scarring, and easy unexplained bruising are among the most recognizable skin findings, particularly in classical EDS.
Joints and Musculoskeletal System
Joint hypermobility — joints that move beyond the normal range of motion — is the hallmark feature of hEDS and HSD. This is often accompanied by joint instability, frequent dislocations and subluxations (partial dislocations), chronic joint and muscle pain, early-onset osteoarthritis, hypotonia (poor muscle tone, especially in children), flat feet, scoliosis or kyphosis, spinal instability, frequent sprains and strains, and temporomandibular joint (TMJ) dysfunction.
Cardiovascular
Fragile blood vessels are the defining feature of vascular EDS and carry serious risk of rupture. Across other subtypes, patients may experience mitral valve prolapse, aortic root dilation, easy bleeding, and low blood pressure.
Autonomic Nervous System and Dysautonomia
Dysautonomia — dysfunction of the autonomic nervous system — is a common and often debilitating feature of hEDS and HSD. The most well-recognized form is Postural Orthostatic Tachycardia Syndrome (POTS), characterized by rapid heart rate, dizziness, lightheadedness, and near-fainting upon standing. Other autonomic symptoms include temperature dysregulation, excessive sweating, and exercise intolerance.
Mast Cell Activation (MCAS)
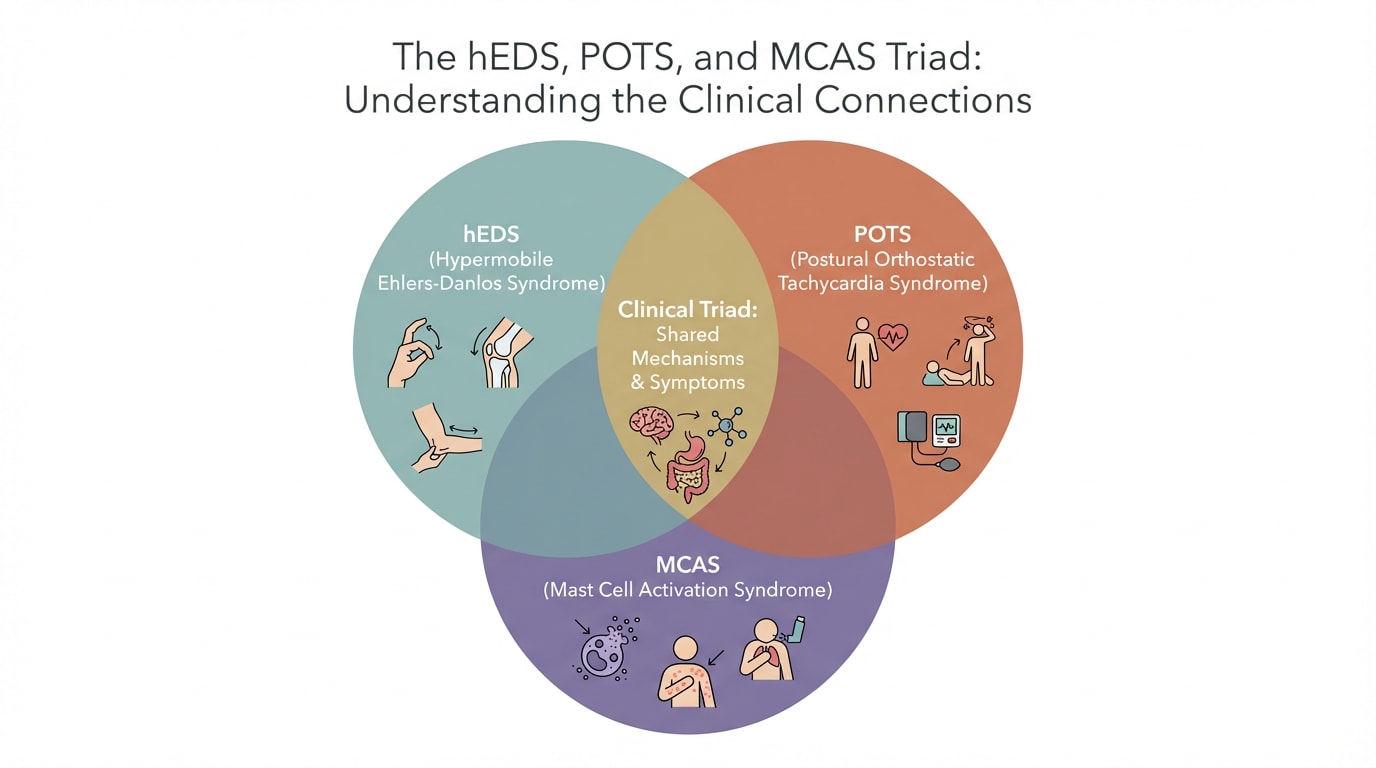
Many individuals with EDS experience Mast Cell Activation Syndrome (MCAS), in which mast cells release inflammatory mediators inappropriately. This can cause symptoms across multiple systems — skin flushing, hives, gastrointestinal distress, respiratory symptoms, brain fog, and hypersensitivity reactions to foods, medications, environmental exposures, stress, and infections. The triad of hEDS, POTS, and MCAS is well recognized in the clinical literature.
Gastrointestinal
GI symptoms are extremely common and include irritable bowel syndrome (IBS), gastroparesis (delayed gastric emptying causing nausea and vomiting), hernias (hiatal or inguinal), biliary dyskinesia, and gallstones.
Neurological
In addition to dysautonomia, neurological manifestations include headaches and migraines (often linked to cervical instability), Chiari malformation, nerve compression syndromes such as carpal tunnel or thoracic outlet syndrome, and small fiber neuropathy.
General
Chronic fatigue — often profound and disproportionate to activity — is one of the most functionally limiting symptoms. Additional findings include myopia and other ocular problems, and in severe cases, pregnancy complications, including preterm labor.
•Impact
Who is Affected
It affects people of all ages, ethnicities, and genders, but is diagnosed more frequently in women. Symptoms often first emerge in childhood or adolescence and may worsen following hormonal changes, pregnancy, injury, or significant physical or emotional stress.
EDS and HSD frequently co-occur with POTS and other forms of dysautonomia, Mast Cell Activation Syndrome (MCAS), fibromyalgia, ME/CFS, autoimmune conditions, anxiety, and depression. This pattern of comorbidities can complicate diagnosis and underscores the need for a comprehensive, whole-person approach to care.
•Clinical Process
Conventional Diagnosis and Testing
There is no single blood test or imaging study that diagnoses most forms of EDS. Diagnosis is primarily clinical and relies on established criteria from the 2017 International Classification of the Ehlers-Danlos Syndromes.
The Beighton Score is the standard tool for assessing generalized joint hypermobility, evaluating flexibility at five joint locations. It is used as part of — but not the sole basis for — EDS and HSD diagnosis.
Genetic testing can confirm most EDS subtypes by identifying pathogenic variants in specific genes (such as COL5A1/COL5A2 for classical EDS, or COL3A1 for vascular EDS). Notably, the genetic basis of hypermobile EDS has not yet been identified, meaning hEDS remains a clinical diagnosis and genetic testing cannot confirm or rule it out.
Supporting evaluations may include echocardiogram (to assess heart valves and aortic root), tilt table testing or NASA lean test (for POTS), gastric emptying studies, skin biopsy in selected cases, and evaluation for MCAS through clinical history, laboratory markers, and response to treatment.
Functional medicine and integrative laboratory testing at GWCIM extends beyond conventional workup to include comprehensive inflammatory markers, nutritional status, hormonal assessment, gut microbiome evaluation, and autonomic nervous system testing — providing a fuller picture of the biological factors influencing each patient's experience.
•Origins
Root Causes and Contributing Factors
EDS is fundamentally a genetic condition. Different subtypes are caused by variants in genes responsible for collagen synthesis and processing, extracellular matrix proteins, and related structural molecules. However, the expression and severity of EDS — how debilitating symptoms are in daily life — is significantly influenced by a range of modifiable factors.
These include nutritional status (deficiencies in vitamin C, magnesium, B vitamins, and amino acids can impair collagen synthesis and repair), chronic inflammation, gut dysbiosis and leaky gut, hormonal fluctuations (symptoms often worsen around menstrual cycles, pregnancy, and perimenopause), autonomic nervous system dysregulation, sleep disruption, physical deconditioning, and the cumulative effects of unmanaged chronic pain and fatigue on mental health. Environmental exposures and mast cell sensitization can further amplify the symptom burden.
Understanding these contributing factors is central to GWCIM's approach — because while the underlying genetic variant cannot be changed, much of what determines a patient's quality of life can be meaningfully addressed.
•Methodology
Our Integrative Medicine Approach
At GWCIM, we recognize that EDS and HSD are lifelong, multisystemic conditions that require far more than a single specialist or a single treatment modality. Our approach brings together functional medicine, physical rehabilitation, pain management, nutrition, mind-body therapies, and mental health support under one coordinated framework — tailored to each patient's specific subtype, symptom profile, and goals.
Care is led by Ashley Drapeau, PA-C, LAc, and Mikhail Kogan, MD, two of the most experienced integrative EDS specialists in the region, working in close collaboration with GWCIM's multidisciplinary team and trusted affiliated providers.
We begin with a comprehensive functional medicine evaluation to understand not just the diagnosis, but the full picture of what is driving each patient's symptoms. From there, we build an individualized treatment plan that may be adjusted over time as needs evolve.
Our focus is on reducing pain and inflammation, stabilizing the joints and autonomic nervous system, optimizing nutrition and gut health, supporting mental and emotional wellbeing, and improving energy, function, and quality of life.
•Expertise
Recommended Providers

Ashley Drapeau, PA-C, L.Ac., MPAS, MAC
Medical Director | Functional Medicine | Long-Covid Program Director

Mikhail Kogan, MD
Integrative and Functional Medicine Physician | ReCODE Program | Chief Medical Officer

Angela Gabriel, MSOM, LAc, SEP
Chinese Medicine Doctor, Somatic Experiencing Practitioner
Misty Embrey, MD
Integrative Psychiatrist

Tiffany Hoyt, DAOM, M.Ac., M.CHM, Dipl. O.M., LAc
Chinese Medicine Doctor

Deirdre Orceyre, ND, MSOM, L.Ac.
Naturopathic and Chinese Medicine Physician, Naturopathic Medical Director

Yael Flusberg, C-IAYT, E-RYT500, RMT, MS
Mindfulness, Somatic and Nervous System Coach | Yoga Therapist | Reiki Master
•Verification
Evidence and Research
•Education
Resources and Insights
•FAQ
Common Questions
EDS is a genetic condition and there is currently no cure. However, many patients experience significant improvement in symptoms, function, and quality of life with the right combination of treatments. Early diagnosis and a proactive, comprehensive approach to management make a meaningful difference.
Because EDS affects multiple body systems and its symptoms can mimic many other conditions — including fibromyalgia, anxiety, IBS, and chronic fatigue — it is commonly misdiagnosed. Many patients, particularly women, are told their symptoms are psychosomatic. Increased awareness among clinicians is improving this, but the average diagnostic delay remains years to decades.
Absolutely. EDS often requires coordination across multiple specialties, including rheumatology, cardiology, gastroenterology, neurology, and genetics. GWCIM is experienced in collaborative care and works closely with your other providers to ensure your care is well-coordinated and comprehensive. We also collaborate with other EDS specialists for unique services.
Your initial appointment with Ashley Drapeau or Mikhail Kogan will involve a thorough review of your history, symptoms, previous diagnoses and treatments, and functional medicine laboratory assessment. From there, we develop a personalized care plan together — one that reflects your priorities, your pace, and your life. Patient education is a cornerstone of EDS care at GWCIM. When patients understand why their bodies work the way they do, they become more effective partners in their own healing.